First flight as a locum medical officer, RFDS Broken Hill, 1966: Bill Pigott
I am a retired medico living in Berry NSW, following a 21-year career with the World Health Organisation. My clinical undergraduate training was at Sydney Hospital and I worked there for 6 years following graduation in 1965.
Dr Norman Rose, Superintendent of Sydney Hospital at the time, was also President of the NSW Section of the Royal Flying Doctor Service (RFDS). In 1966 Dr Rose arranged for selected Sydney Hospital Medical staff members to do locums, while the Service was without a second medical officer. I was privileged to be the first one and was fortunate to be able to do several. As a result, I have had great stories to tell, tales which have been enjoyed by many, particularly those from that first occasion.
 |  |
When I think about those wonderful weeks as a temporary Flying Doctor, I realise what significant things I learned from that experience.
The learning began on my second day in Broken Hill. We flew to Tibooburra in a small de Havilland Drover (an Australian built version of a Canadian aircraft with three engines, one on the nose and one on each wing). Flying across what they call the ‘dead heart’ of Australia.
There were four of us, Jack Jenkins the pilot, Graeme Ambrose the regular Flying doctor, Ted Eslake the dentist and myself. Graeme Ambrose was taking me out to a routine clinic at the Tibooburra Hospital to introduce me to the work I would be doing for the next four weeks while he was away on leave.


 |  |
Seen from the air, the land below us is red. It is almost formless. There are small hills but, on the whole, it is flat and open. We fly across this for an hour and a half or more to reach the small town of Tibooburra.
Working together, the clinic took about two hours. Towards the end, our pilot came several times to the door to ask “have you finished yet?” Dr Ambrose, would reply “No”, and the pilot would respond “Come on, we have to get moving”. He certainly seemed agitated about something. These clinics always ended with a cup of tea and splendid refreshments with the nurses who staffed these tiny hospitals way out in the middle of nowhere. Such morning and afternoon teas were legendary and are stories in themselves.
However, on this occasion, no sooner had we started our tea and sandwiches, Jack appeared and said “We have to go. We cannot waste any more time. No sandwiches. Drink your tea quickly. We really do have to go”. He pointed out through the window, where instead of the clear blue sky of the Australian outback, all we could see was red from floor to ceiling. There was a dust-storm approaching. Jack the pilot says we have to go, so we go.
As we took off from the small dirt airstrip, I realized that this dust-storm was between us and our destination, the base at Broken Hill. We actually flew into the dust, pilot, doctor, dentist and myself the locum doctor, together in the small cabin of this valiant de Haviland Drover aircraft. Jack seemed to be a bit unsettled and soon announced he would see if we could get above the dust. He puts the aircraft into a climb, however as we reach our limit, the engines seem to falter. He announces “We cannot get above the dust, and so we will try to go below it.” By this time, it is clear to me that he has also lost radio contact with our base, and with anyone else. He could not get below the dust either. The dust-storm was down to the ground. For an hour, or so it seemed to me, we flew around, sort of blind, sort of looking for something. Graeme Ambrose explained that Jack was looking for some recognizable landmark so that he could locate our position, but clearly was not finding it. I found myself just looking out the window, looking at all this dust and realizing we were quite close to the ground. Strange and curious. A new experience for me. I suspect I was little bit tense by this time, however I knew this to be so when the dentist, Ted Eslake, well known for his dry sense of humour, says “Look, Jack’s taken his hat off, so he must be really worried”. They explained that Jack Jenkins, a most experienced bush pilot, always wore a hat, and only ever took it off when he was really worried!
As I continued to look out the window, I found myself consciously accepting that there was nothing I could do. I said to myself that he is the pilot, he has the skill to get us out of this. I said to myself that I must let go and let him do what he has to do and get us out of here. I told myself “He has as much interest in getting out of this as I do”. So that is what I did. I remember that I actually relaxed and began to feel strangely calm. Soon Jack found a fence, which he followed and came to a road, which he announced he recognised. He was able to raise on the radio the homestead he knew to be nearby, one with an airstrip. We turned and followed the road, found the airstrip landed safely and spent the night at the homestead.
Since that day, flying in small aircraft has not seemed to bother me, although as a child I hated flying and would get terribly airsick. Later, when working in the highlands of Papua New Guinea, and much later in Nepal, I was often in single-engined aircraft, landing and taking off on some of the most incredible airstrips, but was never worried about flying. I seemed to have a capacity to let go and let the other person, the person whose job it was, take the responsibility for their work. The dust storm had been a significant learning experience for me.

Meeting a patient at a homestead airstrip
The whole four weeks proved to be a wonderful experience for me. As well as going out to conduct small clinics in places accessible by road, where people can physically gather, there were twice daily medical clinics by two-way radio.
One morning, one of the calls was from cattle-station some 200 miles away from the base in Broken Hill. It was the mother of a 15-year-old lad with pain in the abdomen, who was feeling very sick and had vomited a couple of times. It sounded to me that it might be appendicitis. Normally as a doctor one would talk with the patient and do a physical examination. You would feel the abdomen to find out if the pain is localised and where it is most intense. I would have also tested for what is called ‘rebound tenderness’. To do this, you press in on the abdomen and let go quickly. If the pain is more intense when you let go, this is a sign of inflammation within the abdominal cavity. It was not possible for me to do any of this by radio, so I thought, “maybe I can get the mum to do that for me”. Speaking to her on the radio, I asked her was she near the patient. “No, he’s in the other room. Over”. I asked her to test for tenderness with the flat of her hand. She had to leave the radio, go to the patient. She returned to say it was really tender in the lower right corner. I then asked her to press on the lower part of the abdomen and let go quickly. She came right back and said “Yes, he really cried out when I let go quickly. Over to you doctor.” My suspicion is confirmed. I found myself thinking, “Isn’t that interesting. Here is a mother, probably of basic-level education, who is able to elicit a key clinical sign for me”.
The lad will need to come in to the hospital in Broken Hill by plane as soon as possible. I phone the pilot from the radio desk and he tells me we can get out there in an hour and half. I calculate that by the time we’ve got to the plane, fly out and back, and get the lad into hospital, it would be 4 hours or more. This would be long enough for the effects of any pain medication to wear off in time for his assessment by the hospital doctors, which meant he could have something immediately for the pain.
So I now did another thing that would be quite unusual in any setting. I asked the mother, by radio, to go to the medicine kit (which each household has as part of the Flying Doctor Service set-up, containing a range of medications, including injections, each with its own number), to take an ampoule of a particular number, and give a particular amount as an injection into the lad’s upper arm muscle. I was asking her to give her son an intramuscular injection of morphine, to deal with the pain until he got to the hospital.
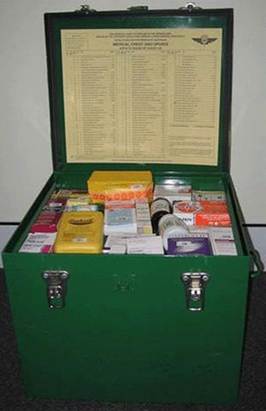

Standard Medical Box
What I had done here was to enable another person take responsibility for what, in a normal hospital or clinic setting, would have been mine. I would have taken all responsibility for the diagnosis, and the initial treatment. However, under these circumstances, we had to share that responsibility. It was a real eye-opener for me to see how much you can, if you have the right setup and you have no choice, actually enable another person take responsibility for what would otherwise be highly professional technical tasks. I was amazed by the extent to which these ordinary folk, out in the country, in these way-out areas in the Australian outback, can with the help of a doctor on a radio, take responsibility for things such as making a diagnosis and administering appropriate medication.
Another example of shared responsibility would occur when radio reception was poor in a particular area. We would start each radio clinic by asking who would like to talk to the doctor, and list the call signs. On several occasions, on reading back the list, someone would call in, saying that they had heard another party trying to call in, and asking would we like them to relay. So the consultation would be through a third party. This was another novel experience for a young doctor from a city hospital.
So the Royal Flying Doctor Service gave me, as a 24 year, old back in 1966, the opportunity to learn some most valuable personal lessons about ‘Responsibility’, letting those who have a responsibility carry out that responsibility and when necessary enabling others take or share a responsibility. I look back and realise my life has been better for having done so. In addition, I discovered the extraordinariness of people we consider to be ordinary.
I subsequently did two more ‘locums’, both wonderful experiences. Later on, when I worked with WHO in Nepal in the 1980’s, building the capacity of Nepalese responsible for training Health workers, I made another Flying Doctor connection. Developing Health Learning Materials and this led us to working with the African Medical and Research Foundation (AMREF), and visiting Kenya for a meeting on Health Learning Materials production. This was an opportunity for me to learn about AMREFs East African Flying Doctor Service.
I discovered another connection much later when my mother spoke about frequent visits of John Flynn, founder of Australia’s Flying Doctor Service, to her home in Mt Lofty when she was a teenager, to discuss medical care in remote areas with my grandfather who was a GP-Surgeon who had practised in Elliston, Peterborough, Port Augusta and from there into the northern parts of South Australia, from around 1912 until moving to Sterling/Mt Lofty in the mid 1920s.

Pilot G Wordsworth talks to the local Police Officer

Published by RFDS in ‘Darn a Good Yarn’. https://www.flyingdoctor.org.au/darn-good-yarn/
