Seeds are sown and from their fields, the results are harvested. Like the lilies of the field, there are so many stories that can be gathered from a person’s life, especially when much of it has been in, as they call it, ‘the field’.
When I worked with the World Health Organisation (WHO), as I did for 21 years, this is the term that the HQ people used to refer to colleagues who worked at country level.
Those of us who worked at country level used the term to refer to activities that took place outside the country office.
And then there were the field trips that filled our lives with so many good stories and so much valuable learning, whether done as a staff member from HQ, or as field staff.
The first three of these are stories that granddaughter Anna would have called “mouth stories” when she was 4 or 5 years old. They have been transcribed from tapes which recorded them as presentations, and used either in a seminar to illustrate a point, or in a course on making presentations. These have been edited lightly for reading. In both cases it was likely the audience would have been mixed, representing different nationalities and a range of ‘mother tongues’. Others were written as “dispatches from the field”
#1:
Standing back, letting go to let another do their job: RESPONSIBILITY
I wonder whether any of you have a fear of flying, or whether you’ve flown very much in small aircraft. Have any of you even flown in small light aircraft? Have any of you been totally lost in a small aircraft?
I have, and I want you to imagine yourself in a small de Havilland Drover (a Canadian built aircraft with three engines, one on the nose and one on each wing) flying across what we call the ‘dead heart’ of Australia. When you see it from the air it is red. It is almost formless. There are small hills but it is flat and open as you fly across it for an hour and a half from Broken Hill to reach a small town called Tibooburra. I was on my way there to help conduct a clinic for the Royal Flying Doctors’ Service, where I was to spend several weeks as the ‘locum’ for the regular Medical Officer while he was on leave.
This was the day after my arrival, and we went together to Tibooburra with the dentist. The clinic took about an hour and a half, and during that time our pilot, Jack, kept on coming to us to ask “have you finished yet?”. We would say “No” and he would say “Get a move on, we’ve got to get going”. He seemed quite agitated.
Now it was always customary at the end of a clinic to have a cup of tea and some sandwiches with the nurses who were really isolated at this very small hospital away in the center of Australia. For them, it was an important social occasion. However Jack said “I don’t want you to waste time. Have your tea, but I don’t want you to have any sandwiches, because we’ve got to go”. He pointed out through the window to a red cloud, from ground to ceiling. It was a dust-storm approaching. Jack says ”we’ve got to go”, so we went.
As we took off, I realized this dust-storm was coming between us and our destination, Broken Hill. We soon actually flew into the dust-cloud. Soon Jack said “ I want to go higher and see if we can get above this. He flies higher and higher until the engine coughs and splutters and we are still in the dust. He mutters “if we cannot go above it, we must go below it”. By this time he had lost radio contact with anyone. He couldn’t get below it because the dust-was right to the ground. So for about an hour we were flying sort of blind. Remember that this was my second day on my first time ever with the Flying Doctor Service. Graeme, the regular doctor who I was to cover for, had taken me out to the clinic, now explained to me that we had lost radio contact with Broken Hill and the instruments to find our location were also not functioning, and what the pilot was doing was looking for landmark he would recognize. It seemed though that wasn’t finding anything. I was beginning to feel a little bit tense myself by now, when I hear “Oh-oh! He’s taken his hat off, he must be really worried”. It was the dentist, who went on to tell me that Jack only takes his hat off when he is really worried. I found myself just looking out the window and looking at this dust and the ground not too far below. Jack soon came to a fence and followed it until he came to and then banked the aircraft and swung round to follow the road.
I remember how at the point in time when my colleague said, “Oh, he’s taken his hat off, he must be really worried now”, as I looked out the window, I became conscious of letting go and accepting the situation for what it was. The process was something like this: There is nothing I could do. I tell myself that Jack is the pilot, and he has the skill to get us out of this. He has as much interest in getting out of this as I do. I must let go and let him get us out of here. So that’s what I did. I take a deep breath and let go. Since that moment, I don’t think I‘ve ever worried about flying in small aircraft. A couple of years later Papua New Guinea, when I was in single engine aircraft landing and taking off in some of the most incredible airstrips, I was never worried about flying, I seemed to have developed a capacity to let go and let the other person take the responsibility of their job. It was a good lesson I think.
# 2:
Enabling another to act when you cannot:
RESPONSE-ABILITY
During those same three weeks with the Flying Doctor Service, in addition flying out to small isolated hospitals and remote cattle stations to conduct routine clinics where people would gather to see the doctor or the dentist, you conduct a medical clinic by radio from the Base twice a day.
One morning, a woman on a cattle-station some 200 miles away from the base had called in to say that they had a 15 year old who had pain in the abdomen, had been feeling very sick and had vomited a couple of times. It was the boy’s mother who made the call on the two way radio. I gathered information about the onset and nature of the illness. Then I asked her -was she near the patient; She said “No, he’s in the other room”. When, as a doctor, you’re think you might be dealing with appendicitis, there are some things you look for. if you press in on the abdomen and let it go quickly, the pain is even more intense, it’s called rebound tenderness. If that test is positive it means that there is inflammation within the abdominal cavity, and I thought, ‘Maybe I can get her to do that for me’. So I described how to do it, to press in and let go quickly. She had to leave the radio, go to the patient bedside. When she came back, she said “Yes, he really cried out when I let go quickly”. My thoughts were ‘isn’t that interesting, here is a mother, probably of basic-level education, who is able to elicit an important clinical sign for me.
It was clear now that he had to be brought in, so I rang the pilot who said we could be out there in two hours to pick up the patient. I worked out that it would be at least 4 hours before he was back into the base and to the Broken Hill Hospital for treatment, and that time would allow for some pain relief that would wear off by the time the hospital doctors would see and assess him. For that I would do something which is quite unusual in any setting. I asked the mother to go to her medicine kit (the one that is part of the Flying Doctor’s Service set-up and to take and ample of No.40 and give 15mils of that as an injection. What I was asking her to do was to give her son an injection of morphine to deal with the pain until he got back into the hospital. Now it seemed to me that what I was doing here was letting another person take responsibility for what would in a normal hospital setting had been mine. If I was there at the bedside, I would have taken all responsibility for that. So this was a real eye-opener of how much, if you’ve got the right setup and you have to you can actually let another person take responsibility for what would otherwise be highly professional technical tasks. I was amazed that the extent to which these ordinary folk out in the country areas, in these way-out areas in Australia could take responsibility for things like making a diagnosis with the help of a doctor on a radio and giving drugs. So the 2nd thing that was a lesson for me in the Flying Doctor’s Service was letting people take their and enabling people to take responsibility.
I was in Norway some years later, and came across a haematologist who had patients who lived in remote and isolated areas of Norway. They were taking anti-leukaemia drugs which kill the leukaemia cells, but also affect the level of normal white cells in the blood. The size of the next dose of drugs depends on the patients white-cell count. Because of their isolation, especially in winter, he had taught his people to do their own white-cell counts. His view was that because their life depended on it, they would do it properly. From his experience, they did so. I was fascinated and when I returned to Australia and told this story to two haematologists that I had earlier worked with, they were furious with me for even telling the story, They angry because, as they said “ you simply cannot let people take that sort of responsibility”.
Interesting. What about you? Are you able to let people take responsibility for the job they have? Perhaps more importantly, are you able to enable others and to let others take responsibility for the things which they can do but which they are often not allowed to do?
# 3:
PERCEPTIONS: Is the glass half full or half empty?
I wonder how many times a day you drink from a glass like this. (a glass on the table, It is half full of water). Often? I see that you do, and I’ll come back to that.
I remember a time when I was working with a group of young parents, when one of the mothers was complaining about the way her child always left her room in a mess and even left the yard in a mess, when the child had been playing in the yard. Have you come across people like that? I wonder what your reaction would have been when you found out that the child was less than 2 years old.
When I came from ‘the field’ to WHO Headquarters, it wasn’t long before I heard people talking about 2 particular WHO Country Representatives (WRs) as being extremely hopeless. Have you ever heard that comment about WHO Representatives? I wonder then what your reaction would have been when you met those 2 WRs in a WR Seminar and discovered that ever since that they had been in their jobs as WRs, they had experience ongoing civil disruption and political upheaval of the sort that meant there was a new Minister of Health every six months. (I was to experience this myself as a WHO Representative back in Nepal some years later, and understood how change of government and change of Minister of Health could disrupt WHO’s programme of work with the officials of a country.)
Recently I was reading a book by Steven Covey who writes about personal development and leadership. In it he tells the story of how he was riding in the New York subway when a man got on the train with three children and sat next to him in the only available seat. The man sat very quietly and was very still while his three children behaved in a way disturbed the rest of the passengers on the subway car. Even Steven Covey got very irritated and said to himself “Somebody should tell the man that his children are mucking up and disrupting others”. Not before long did he realize that he was going to be the one that should tell him, as the man with the disruptive kids was sitting next to him. I wonder what your reaction would have been when you heard the man say “Oh, I guess they’re being disruptive because we’ve just come from the hospital where their mother died an hour or so ago, and I am at a loss what to do”.
I have told these three stories about changes in perception because, for me, the really important thing about my work, about staff development and about my role as a parent, is the need to help people look at both sides of a picture, to encourage people not to make assumptions, and to enable them to go beyond the obvious and to look for the view from the other side of a situation. Do you think those are valid conclusions to come from three stories like that?
I believe we can learn from such stories. I’d like to identify lessons, even tools which can be used by all of us in our work and in our life in general. I’d like to start by going back to the mother who expected her two year old child to be keeping the room tidy. (Incidentally we asked her what about her husband: “What was the husband’s workshop like?” , she said “Oh, it’s a terrible mess” . We asked what about the laundry and other places in their house, and she said “Oh, they’re terrible mess too”)
The setting in which I heard his mother complaining about the fact that her two year old child could never keep the room tidy was a community based programme on “parenting” in which we were working with young new parents to help them look differently at their role as a parent .
The reason why we were together was that we had been asked by the Infant Welfare Agency in Adelaide, the city in which I was living and working at that time, to set up some programmes for young parents on “Parenting”. The reason was that there were young parents living in new housing areas where all the residents were young parents with young children. There were no older people, no points of reference, no models of parenting. These young people were isolated, alone and comparing themselves with each other. They punished their children to make them behave, and some of the children were appearing at a local clinic damaged, so we were asked to do something about it. The attitude of the mother who wanted her 2 year old to have a tidy room was typical of what these parents felt. They thought the answer was to punish the child for such untidiness. Our job was to help them to look at things differently.
The courses were held over a period of six weeks, one night a week for six weeks. We could ask them to do something as homework between sessions. We started the course with discussion on the’ Joys and sorrows’ of being a parent, and moved onto a second session on the stages and milestones in early child development, leading up to a third session on the issue of Discipline. We wanted to present a constructive developmental view of ‘discipline’. Clearly we needed to explore their understanding of the issue, so we asked them to define in their own words what they meant by ‘discipline’. They did this in small groups and reported their definition back to the whole group. They all said “our job as parents is to make these children good”. Whatever words they used indicated that they believed that children were born bad and now had to be made good. This alarmed us. We had set up the course to guide them to see discipline a constructive tool to help the child learn responsibility and life skills. We realised that we could not simply tell them that there was another way of seeing it or what to do differently. We had to enable them to see things differently. So on this first occasion we went into a huddle and revised what we had planned as the ‘homework’ for the week. We asked them for following week to take a sheet of paper, draw a line down the middle and on it, at the end of each day, write down two good things their child had done and two bad things, and come back next week and tell us what happened. We were surprised by the response. The following week everybody arrived early. They were all excited. When we asked them what had happened, the answer was that “at the beginning of the week we could hardly find anything good about the child, but by the end of the week the child had changed”. This response was consistent over the several years that we ran these programmes. So interesting!
Can you see the connection then with my first 3 examples? It seems that people find what they look for, and by encouraging and enabling them to look for something different, change happened. Their perception changed, and change happened.
At the same time, my real work was working with students from different health professions, setting up an educational programme where they were to learn to work together. One of the courses was for students in their 2nd year, working in small mixed groups with some students from medicine, some from nursing, and others from social-work, occupational therapy, physiotherapy and psychology.
On the first day of this course we asked “ What does your profession do in a particular health situation?” , wanting them in their mixed groups to tell each other what they do as members of their profession. In the first year of this experimental programme, when the question was posed, nothing really happened. The sort of inter-action that we wanted between these people just did not happen. We hoped they would establish a foundation on which they could look into teamwork as a positive thing for them to do. We had an evaluation of first course management committee, which included the heads of the schools of each of these professions. When we told of our disappointment, it was the head of the school of social work who said “You asked them the wrong question. With that question you could not have expected to get any more”. I replied “What question would you ask?” He quickly responded “You should have asked them what they’re trying to achieve”.
So the following year, we did ask them, at the beginning of the course, to share with each other what the, as members of their profession, were trying to achieve. The difference was dramatic. It was the most exciting opening up of these students. Once they began to talk about what they were trying to achieve, they discovered that had much in common and recognised the unique contributions they also would make. It made sense to them to be different and to have different offerings and to work together.
I came away from these experiences with two tools; one was a question and other a framework.
The question is “what are you trying to achieve?” The framework is similar to the one we asked our young parents to use, identifying the positives, the strengths in the present situation, and separately listing the negatives, the weaknesses. It is a framework to look at the good and the bad, the strengths and the weaknesses, the ‘pros’ and the ‘cons’, helping factors and hindering factors, resilience vulnerability.
Using such a framework helps me understand how it is that I can be successful in achieving what I wish to achieve. I look at the positives or the strengths within my present situation which will help and I can see the things that might prevent me from achieving what I want to achieve. This gives me a very quick problem-analysis of the present situation which makes it more likely for me to achieve what I want to achieve. I’ve looked for the strengths, I’ve looked for the positives, and I’ve identified which ones I can build on. I’ve identified some of the constraints, some of the negatives and can identify which are worth addressing, which to move away from or just leave alone. For me, these have been two very successful tools. The value of the question has increased as I subsequently worked in Nepal with WHO and as I worked in the Staff Development Programme in WHO headquarters.
One example from Nepal in the 1980s comes to mind. A group of students came to me in my office in Kathmandu. They were medical students, senior medical students, who wanted to set up a clinic in one of the villages on the outskirts of the Kathmandu valley. They said they wanted me to help them. I suspect they wanted me to tell them how to go about it. I thought for a moment. Quite sincerely, I wanted to clarify with them what it was that they wanted to achieve by setting up this clinic. Equally, and as sincerely, I did not want to just tell them how to do it. I wanted to help them work it through for themselves. So the first thing I said was “Please help me understand what it is you are trying to achieve”. I asked my first “question”. They began to tell me what they want to do. “No”, I say, “What do you want to achieve”. Again they say what it is they intend to do. So I ask them what will be different if I go to that village in 5 years time. “What will I notice?” , I ask. This led to a great discussion, more between themselves than between me and them. They debated exactly what it was that they were going to try to achieve. They wanted something for themselves. They wanted something for the village. They wanted something for other students to be involved in. Once we clarified that, we then continued with my next ‘question’. I asked them “What are the good things about the present situation which will help you to achieve what you wish to achieve?”. “In the present situation, now, as far as that village is concerned, and concerning what you’ve already done, what are the things that are helping you?” On the other side, what are the things that might prevent you achieving what you want to achieve? what are the barriers?, what are the blocks?, what are the negatives?” This led to further lively discussion and I could now say to them that I understood both what they wanted to achieve and something about the setting in which they would work. I summarised what I had heard and asked them how I might be of assistance. “You have helped us so much already,” they said. My student friends seemed to be pleased and thanked me for my help. I was pleased that I had helped them help themselves.
In the training programme on “Presentation Skills”, we were also using these two tools. In preparing speeches or presentations, we were being encouraged to ask ourselves “ what do we want to achieve by giving a talk, by giving a speech or making a presentation?”. Then we were giving short presentations which were videotaped and critiqued by identifying what are strengths, what are the good things in what we do and what are the things that we can improve on, what are the things which are hindering us getting our message across. This is another example of the application of these two tools.
Another area where these tools may be used, and I throw this as a challenge to those of you who are dealing with them at the moment, is the situation budget cuts within our programmes. I often wonder why people’s immediate reaction to a budget cut is to fall flat, get depressed and say there’s no hope of doing anything, because I haven’t got any money. I think an alternative would be to say, “What is it that I’m really trying to achieve?” and “What is it in my present situation that helps me to achieve that, even though a negative is going to be the budget cut?” So in a sense, there are some applications of these two tools even to the budget cuts that we are facing in the Organization at the moment. I can see from your faces that this might be a little more difficult for you do under the circumstances, however I am willing to try.
This sort of thinking isn’t new. If we were to take the positives as being the light in a situation and the negative as being the dark, we can see that the parents in my earlier story were only looking at the darkness. They were punishing their children to eradicate the badness, to get rid of the darkness. I’m suggesting is that if we look at the light, it will help us to see the situation as a whole. This reminds me of the old Chinese saying which says that just lighting one match can get rid of the darkest of darkness.
It is my view that if we cultivated the attitude of looking at the positives and the negatives we would be better able to bring about change. Instead of trying to eradicate the darkness, we can just turn on the light, and so produce change.
This brings me back to the glass of water. Is it half-full or is it half-empty? I believe that the way we see it, our perception of its fullness , or emptiness, will influence the action we take. Perhaps it will be more significant when there is even less water in the glass. Personally I would rather focus on the ¼ fullness than to become overwhelmed and depressed by the ¾ emptiness.
So I would like to leave that with you as two tools. “What can I achieve?” and “Can I look at the good things, the bad things, the strengths and the weaknesses” as tools for helping myself, for helping yourselves and for helping others to help themselves. Do you see the link?
____________________________________________________________________________________
#4 :
CAMBODIA FIELD TRIP, May 2000: ( For the WHO HQ Staff Newsletter )
I returned from a four-day field trip with the Secretary of State for Health and the Acting Director of the Planning Division. We had visited three provinces and included on our itinerary 5 hospitals 5 health centres, a Regional Training Centre, two Provincial Health Departments, a Trauma Centre, an orphanage and a pagoda or two. .
Three images stand out:

1: If you think you are unlucky or having a hard time, consider this nine year old, who fell from a tree, onto a landmine which exploded. Bad enough luck to fall from a tree, but to fall onto a landmine!! He lost the lower part of one leg and has extensive injury to the other, yet the hospital staff of the NGO Emergency Centre in Battambang say he is the brightest of their people and is an inspiration to everyone.

2: This farmer three days earlier stepped on a landmine in one of his own fields. He has had a below knee amputation. Imagine what that will do to his ability to support his family.

3: These children suffer from diarrhoea or malaria. These are the lucky ones who have reached the hospital in Pailin. Many do not. Others find the drugs they buy over the counter are labelled mefloquine, but are actually fake.
So my message to those who do so, stop complaining about how difficult things are and how much work you have. Be thankful for your own health and the opportunity we all have to work towards meeting the needs of such people. Be encouraged by the news that most of the people I met are getting on with their work and benefiting in a variety of ways from support WHO from all levels is giving through staff work and technical collaboration with the Ministry of Health in Cambodia.
Do not moan about how life is for you. Do what you can for others. The people out here need all our support. We each have purpose in this life, and working for WHO is a great opportunity to contribute to the health of hundreds and thousands of people in the remoter parts of the world.
Let the lad who fell from a tree onto a landmine and the people who work in outlying Health centres with only the most basic of equipment and a positive attitude, be an inspiration to us as well.
____________________________________________________________________________________
#5 :
The Martina Hingis visit to Nepal, February 1998
Observations by Bill Pigott, WHO Representative to Nepal
Martina Hingis, the world’s number one woman tennis player and WHO Goodwill Ambassador for Immunisation, visited Nepal on her way home from winning the Australian Open and reaching the final of the Pan Pacific in Tokyo. Martina, her mother and a family friend came on a ‘private visit’, during which they wanted to trek and also visit the site where a donation of $10,000 from Martina had funded an immunisation campaign against neonatal tetanus. We at the WHO Nepal office were asked to facilitate the arrangements and suggested a programme that included a half day ‘trek’ in the mountains outside Pokhara, a night at Tiger Tops in the Chitwan National Park, and a morning visit to immunisation activities in the Nawalparasi District, which is just across the river from Chitwan.
Dr. Jagat Giri, the District Health Officer who so impressed me when I observed the second round of tetanus immunisation for all women of child bearing age (14 to 45 years) the previous May, was delighted at the prospect of a visit, and organised for the third round of immunisation to coincide with Martina’s visit. He also arranged that routine child immunisation would also be done and orchestrated the most amazing welcome by the villagers at the three immunisation centres we visited.
The Hingis party arrived from Tokyo via Shanghai on Wednesday evening. Many recognised Martina, and wanted photographs and autographs. It was amazing to see airport staff produce any scrap of paper, including banknotes for autographs.
DAY 1 Thursday 12 February;
While the Hingis party, together with Drs Anton Fric and Imam Mochny of WHO, fly from Kathmandu to Pokhara, enjoying spectacular mountain views on the way, with Martina in the cockpit for some of the journey, my wife Leslie and I drive in our own Land Rover Discovery, leaving early in order to be in Pokhara before they arrive. After lunch we drive out to Lumle, but sadly the high mountains have clouded over.
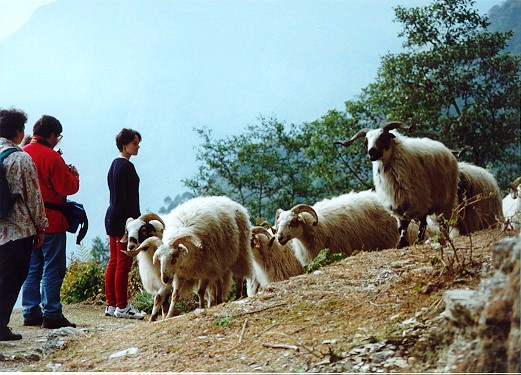
We then walked from Lumle to Chandrakot, about an hour or so away. The walk through the villages was wonderful. The clouds obscured what are usually spectacular views of the Annapurna range, but the terraced fields of green new wheat and yellow mustard flowers were brilliant. Martina wanted to meet Tibetans.. and she did, selling handicrafts in one of the villages. We encountered women carrying heavy loads of fodder, lots of children, and a large flock of mountain sheep.
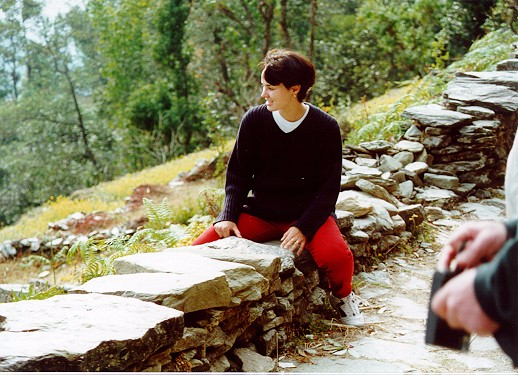
Martina rests during the walk from Lumle to Chandrakot photo by Bill Pigott
As we walked, we talked about village life, about health, the importance of women’s literacy, the importance of population control, the vicious circle of high child and infant mortality creating the desire for more children, the pressure of this on child survival, population growth and land usage, and the contribution of all this to poverty. We discussed the importance of immunisation and basic prevention of illnesses. At the village water tap, we talked about the importance of a clean water supply and the immense burden borne by the women of Nepal spending hours each day carrying water in places where there is no pump or tap. Martina was clearly most interested.
Day 2: Friday 13 February
Before we set out from the Fish Tail Lodge for Chitwan, Martina was able to meet a few of the many young tennis players of Pokhara. The four hour drive to Chitwan allowed them to see more of the country, the roadside farming activities and village life. We had a coffee break along the way at a riverside stop, and were able to watch a man ploughing his fields with a traditional wooden plough and two buffalo. (We carried thermoses of hot water, tea, coffee, cookies and brownies with us and discovered how much Martina enjoyed the brownies made by Gopal our cook, which are such a favourite of our boys.).

As we arrived at Chitwan, there were army parachutists doing practice jumps at Meghauli airport, just beyond which we left our vehicles to cross the river by boat to Royal National Park, for the twenty minute drive through the jungle in an open Land Rover to the Tiger Tops Lodge.
There we were assigned to our rooms, had a late lunch under the trees and then went for a two hour elephant ride to see the wildlife, which included rhinos with babies, wild boar, deer and hog deer and lots of birds. Afterwards Martina rode an elephant herself, and fed the baby elephant they have there. Then there was time for a drink and a slide show before dinner. We had great conversations with Martina about what it is like to be on the tennis circuit, and her love of horse riding.
Day 3; Saturday 14 February
The third day started early, with a misty morning drive for 20 minutes in the open Land Rover through jungle shrouded in morning fog, during which we encountered beautiful herds of chitral deer. As we reach the river which we must cross to reach our vehicles, we are met by a Star TV crew, already filming, and this starts the day a little “on edge”.
We pack the two vehicles and drive for an hour on rough roads to the main highway, cross the wide Naryani River to the District of Nawalparasi, where we are welcomed by a banner across the highway and the district officials, who each present Martina with a posy of flowers. We then move off in convoy to visit the three immunization centres, all of which are along the highway.

The village welcomes were quite overwhelming. At the first stop there is a real crush as everyone tries to place their garlands of flowers around Martina’s neck. She stops and greets them all, but there is some pressure and the police seem to find it difficult to maintain a path to the Primary Health Care centre, where the immunisations are taking place. However, the police wisely bring the WHO Land Rover to the door of the PHC centre, and as Martina leaves, we stand amazed at the spectacle of people showering the vehicle with flowers as she drives back to the highway.

Crowds at Choramara greeting Martina Hingis photo by Leslie Pigott
The second stop was at a school in Arunghat, where the children lined up across an open field, so the pressure seemed less. It was wonderful to walk through the lines of children with their banners, clapping and placing more garlands of flowers over Martina’s head. Here we heard the first of the welcome songs in English. Martina seemed to love every minute and responded to each person.
The third stop was at the Health Post in Dhumkibas; again with crowds of people lining the path, clapping, and garlanding Martina with flowers. In the grounds of the health post, they had arranged some chairs and a small table with the photographs of each of Their Majesties the King and Queen, each with a garland of flowers, which are the custom for official ceremonies in Nepal. Once the crowd was seated, the speeches of welcome and ”thank you” began. The ceremony ended with a shower of gifts and a visit to the immunisation centre. I loved the way Jagat Giri addressed the crowd as my brothers and sisters. Martina gave a wonderful speech of thanks.
The whole morning was truly amazing. What an outpouring of affection and gratitude! Martina just glowed. It must have been quite a magic moment for the village folk, but also for Martina. I was really touched as two elderly women came up to Martina during the ceremony and offered their ‘flowers’, one just a single flower and the other a tiny bunch of leaves, offered reverently in their outstretched cupped hands.

I realised, as I sat waiting for my turn to say a few words, that it is rare for people in developing countries to meet, in person, the one who has funded an activity. And even more rarely is it a 17 year old tennis princess. This is another aspect of Development with a human face. What a wonderful young face. What a privilege it was to have been part of such an event.

Listening to speeches and awaiting immunisation against Tetanus at Dhumkibas
photo by Leslie Pigott
Immediately after the ceremony we set out for Kathmandu, stopping for lunch on the way. What a sparkling day on which to make that journey, beautiful on any occasion, but particularly so today, as we followed the Naryani and Trisuli Rivers and climbed up into the Kathmandu valley on a beautiful spring afternoon.
We arrived back in Kathmandu by 5 pm. Sadly, we were asked to excuse Martina from attending the reception planned for later in the evening. This was to have been the opportunity for her to meet the young tennis players of Kathmandu, so we cancelled their attendance, and proceeded to have drinks and snacks with the WHO team who had supported the visit, together with others who had been invited and still wanted to hear about the visit. I was pleased Martina was able to meet the young tennis players in Pokhara, and some others who turned up at the airport on the morning of her early departure for Switzerland. I feel that the visit went well. The Hingis party seemed very happy as they left, however I sense that they were quite overwhelmed by the outpouring of affection and the crowds at the immunisation centres in Nawalparasi, and I think a bit ‘culture shocked’ by their first exposure to village life in a third world country.
Our biggest concern had been how to maintain the privacy of the first two days of the visit. Somehow we managed to contain most of the press activities to the official day. The report on Star TV news, which went out on Sunday evening to more than 50 countries, was excellent and positive. We were able to take some good photographs. We had good front page press coverage in the local press, of both her arrival and departure. The information sheet prepared by us has been picked up by several of the local papers.
 photo by Leslie Pigott
photo by Leslie Pigott
Eddy Risch, a photographer from Blick, the Swiss newspaper, also accompanied the visit. Mario Widmer is a close friend of Melanie Zogg, the mother of Martina, and as sports editor of Blick will do a story with Eddy Risch’s photos. Mario and Eddy were the third and fourth members of the Hingis party for the visit.
Eddy took an enormous number of photographs and seemed to indicate that some could be made available to WHO. He was a great travelling companion and gave us lots of information about life on the tennis circuit and was delighted with and enthusiastic about everything he found in Nepal (except the way the local drivers drive!). However I think Martina’s mother and Mario Widmer were rather overwhelmed at times. Martina took everything in her stride, except for the cameraman and interviewer from StarTV.
As they departed from Nepal, they were all really appreciative of our efforts, and recognised that the full impact of the visit on them may not be realised for days to come. We could not have done it at this end without Anton Fric, a WHO staff member in Indonesia who had played competition Tennis with Martina’s mother years ago, who was able to act as interpreter for Melanie, and be the key liaison with Martina herself. We could not have done it without Dr Ojha from the Department of Health Services, Dr Giri, the District Health Officer in Nawalparasi, and his team of health workers and volunteers.
We appreciate the presence of Dr Mochny representing the WHO South East Asia Regional Office, and in retrospect are relieved that we did not have to deal with a larger or higher level team under the circumstances. (It had been proposed that the WHO Regional Director also accompany the visit.)
My who team here were magnificent, especially Jorge Luna, Patricia Brice , Lava Shrestha and Narendra Tandukar, and I am most grateful for the role my wife Leslie played, sharing the driving of our personal Land Rover, which was one of the vehicles used, and being particularly helpful in explaining to Martina different aspects of Nepali culture. The other WHO drivers, Narayan Sapkota and Ram Ranjit were an essential ingredient for the success of the visit.
This seems to have been the first visit of a WHO Goodwill Ambassador to a country to observe immunisation activities. It was a great experience. We were all moved by Saturday’s events in the villages and Martina’s gracious response. She was treated like royalty, and responded accordingly.

photo by Leslie Pigott
